Nasal liquorrhea (NL), the discharge of cerebrospinal fluid into the nasal cavity, is a rather rare but potentially fatal disease that is not always correctly diagnosed by doctors and can exist for many years under the guise of allergic or vasomotor rhinitis. Cerebrospinal fluid fistula (a channel through which fluid drains) occurs due to a defect in bone structures and meninges. If the bone defect is large, the membranes and the substance of the brain can fall through it, creating a herniated sac called meningo (encephalocele).
Forms
Such a fistula can form as a result of a craniofacial injury preceding surgery in the nasal cavity and on the base of the skull. Or spontaneously, against the background of increased intracranial pressure. Thus, traumatic and spontaneous nasal liquorrhea are distinguished. In turn, spontaneous nasal liquorrhea can be congenital, as a result of intrauterine disorders in the formation of bone structures at the base of the skull, or acquired. In the latter case, a fistula can form against a background of various problems. These include metabolic disorders, increased weight, increased intracranial pressure, developmental abnormalities of the anterior parts of the base of the skull, etc.
What is the danger?
In itself, excessive discharge of fluid from the nose is quite unpleasant, as it seriously reduces the quality of life. But a more serious complication is meningitis, i.e. inflammation of the membranes and substances of the brain, since there are conditions for infection to enter from the nasal cavity into the cranial cavity in any case of colds. Another serious complication is pneumocephaly, when air enters the cranial cavity through an open fistula. These complications require emergency hospitalization of the patient.
Symptoms
Symptoms of profuse nasal liquorrhea:
When the head is tilted, a clear, light liquid is released from one half of the nose.
Latent, recurrent nasal cerebrospinal fluid is more difficult to diagnose and requires the use of the entire arsenal of laboratory and radiation techniques. In the supine position, a cough occurs, as the cerebrospinal fluid flowing into the oropharynx can enter the lower respiratory tract, causing reactive laryngitis, tracheitis, and even pneumonia. Cerebrospinal fluid complicated by meningitis is manifested by a wide range of neurological disorders
.
A patient with nasal cerebrospinal fluid usually has a history of traumatic brain injury, or surgery involving the nose and paranasal sinuses, including endoscopic surgery. In this case, spontaneous nasal liquorrhea may begin suddenly for no apparent apparent reason.
Diagnostics
 First of all, the doctor determines the nature of the discharge:
First of all, the doctor determines the nature of the discharge:
The picture shows a visual examination of the patient. When the head is tilted down, a clear liquid begins to flow out of the nose.
Nasal liquorrhea is often mistaken for rhinitis (allergic or vasomotor). It can also remind patients of the condition when the nose is irrigated with liquid medicines.
Profuse nasal cerebrospinal fluid can stop on its own for a while, while patients experience headaches due to fluctuations in intracranial pressure.
Damage to the anterior parts of the base of the skull may indicate:
 The standard examination should include:
The standard examination should include:
-
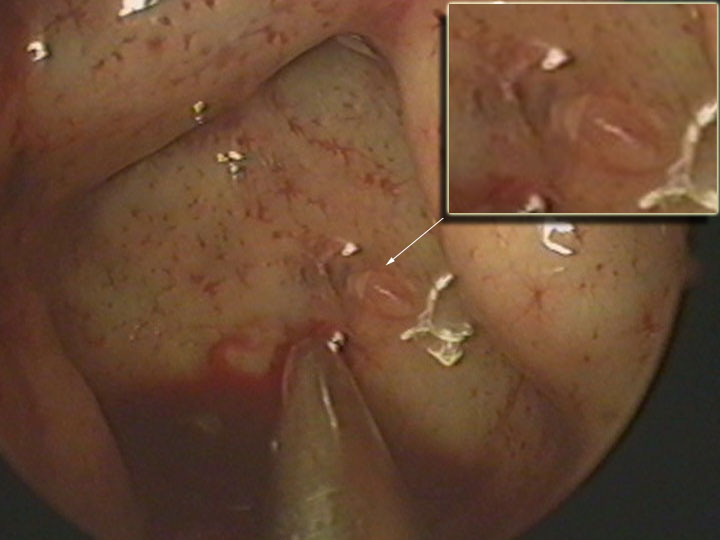
Endoscopic examination of the nose and paranasal sinuses (the picture shows an endoscopy of the nasal cavity with a direct endoscope; in the projection of the posterior wall of the sphenoid sinus, a small bone defect is visible through which cerebrospinal fluid enters).
-
Rhinoscopy.
-
Hearing examination for the presence of ear liquorrhea,
-
Neurological examination,
-
Biochemical analysis of liquid nasal secretions for glucose levels, determination of CSF-specific proteins (beta-2 fraction of transferin, trace protein).
 Radiation diagnostic methods:
Radiation diagnostic methods:
-
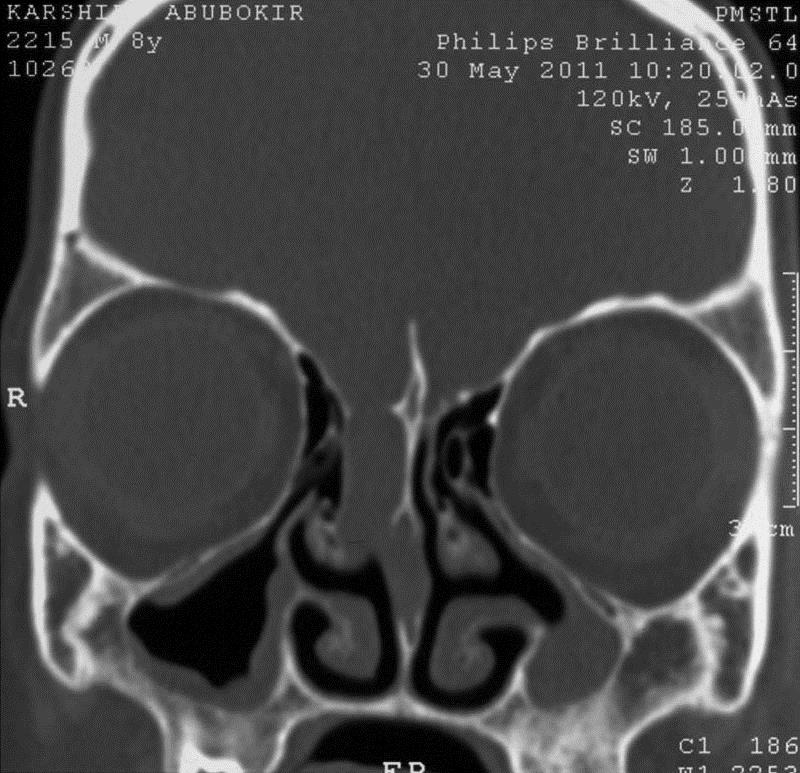
Computed tomography (CT) of the base of the skull and paranasal sinuses (the figure shows a large defect in the base of the skull in the projection of the sieve plate with the formation of a meningocele (shown by the arrow)).
-
CT cisternography with endolumbal contrast injection to more accurately determine the location of the defect at the base of the skull. This study is performed in a hospital setting.
-
CT scan of the skull and brain to exclude hydrocephalus, neoplasms of the base of the skull, and detection of meningocele.
-
Magnetic resonance imaging (MRI) is an adjunct to CT to rule out meningoencephalocele.
-
Cerebrospinal fluid-sensitive MRI. It is a non-invasive method, has no radiation load and takes a little longer than conventional MRI.
Treatment
The treatment of nasal liquorrhea is mainly surgical. For many years, it required severe, sometimes disabling interventions on the base of the skull using transcranial accesses. Over the past three decades, the development of endonasal endoscopic surgery has radically changed the situation, and now most cases of nasal cerebrospinal fluid can be cured by gentle minimally invasive interventions performed without external incisions through the nasal cavity under endoscopic control, which allows the surgeon to significantly improve the view of the surgical field. The endoscope helps the surgeon to determine the location of the cerebrospinal fluid fistula, carefully separate the mucous membrane from the bone defect and accurately place the graft at the site of damage.
The method of surgical intervention is determined jointly by an otorhinolaryngologist-surgeon and a neurosurgeon. In some cases, neurosurgical intervention is required. For example:
-
Large or multiple bone defects.
-
Traumatic brain injury with compression of the brain.
-
With increased intracranial pressure, when fistula surgery cannot be performed before hypertension is eliminated by bypass surgery.
-
With a complex fistula location.
Treatment of nasal liquorrhea is primarily aimed at restoring the barrier between the nasal cavity and the intracranial space so that an intracranial infection does not develop. At the same time, soft tissues, rather than bone fragments, can be used to repair small defects in the base of the skull. However, in case of major bone defects, they must be covered with a dense cartilage graft so that an encephalocele (cerebral hernia) does not form.
Postoperative period
After surgery, patients are usually advised to follow the following recommendations: avoid excessive physical exertion, prolonged exertion, and forced coughing. The regime should be as gentle as possible. Try to stay in a supine position as much as possible, and lift the head end of the bed. If the signs of nasal liquorrhea disappear completely, the patient is discharged with recommendations that must be followed for at least 6 weeks.
It is recommended to carefully remove some of the tampon fragments from the nasal cavity within 3-10 days after surgery. In this case, the absorbable materials located directly near the graft remain and are removed later. For the entire postoperative period, antibiotics are prescribed in doses that prevent the development of sinusitis.
In the late postoperative period, an endoscopic examination is performed every time a patient visits to rule out recurrence of the encephalocele, especially if a large defect has been repaired. It is important to carry out differential diagnosis of rhinoliquorrhea with allergic, vasomotor and viral rhinitis in the future.
Summary: thus, nasal liquorrhea is a rare but quite dangerous disease that can lead to serious complications, including meningitis and pneumocephaly. The differential diagnosis of rhinitis is not always simple and unambiguous, therefore, a timely correct diagnosis is the key to adequate treatment. In view of the above, an examination by a specialist is the first and necessary step in diagnosis. If nasal cerebrospinal fluid is confirmed, minor surgery is necessary to restore the integrity of the skull base.










.webp)




.webp)

