

Bariatric surgery - narrowing of a part of the stomach
Operations that narrow the lumen of the stomach are called restrictive in surgery. The name comes from the Latin word "restrictio", which means "restriction". Currently, two types of restrictive operations are mainly used.:
These operations use the same weight loss mechanism. What is this mechanism? There is a special area in the stomach that is located below the junction of the esophagus with the stomach.
-
Gastric bandaging (placing an adjustable restrictive ring on the stomach).
-
Sleeve gastroplasty.
This area contains saturation receptors– special cells that send signals to the brain that the stomach is full and that you need to stop eating. These cells are excited when the stomach wall stretches. Under normal conditions, such stretching occurs only after the food fills the stomach and reaches the level of this zone.
Restrictive gastric surgeries use exactly the work of these receptors.
Gastric bandaging
During this operation, an adjustable ring is placed around the upper part of the stomach, and it takes on the shape of an hourglass.
The "Small ventricle" located above the ring has a total volume of
10-15 ml, i.e. it is enough for a person to eat only one tablespoon of food so that it fills the "small ventricle". The stomach wall stretches at this point, and the saturation receptors begin to send a signal to the brain "enough, I'm full." Thus, a person simply cannot (and most importantly does not want to) eat a lot of food, and naturally begins to lose weight. Such an operation to impose an adjustable restrictive ring is now very popular in the world, especially in Europe. The exact name of this operation is "laparoscopic gastric bandaging".
Today, it is used as a restrictive ring;
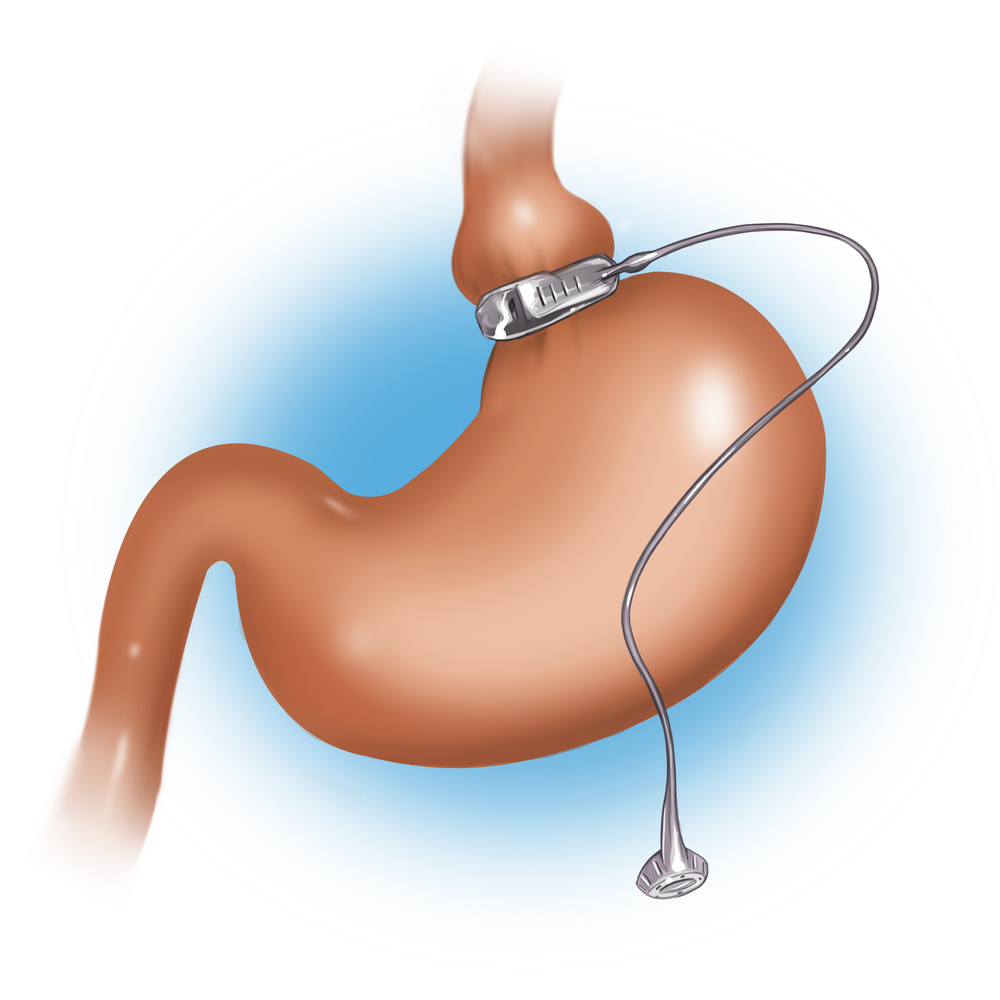
only an adjustable silicone bandage with an internal hydraulic cuff. In the postoperative period, fluid is injected into the cuff cavity through a special adjustment port implanted under the skin. This is necessary to accurately calibrate the ring for each patient: we are trying to achieve a narrowing that, on the one hand, will ensure the retention of solid food above the ring, and on the other hand, will freely allow water and other liquids to pass through. The introduction of fluid into the cuff is a procedure called adjustment. Making adjustments is an essential condition for weight loss after gastric band surgery.
Advantages of gastric band surgery compared to other bariatric surgeries
-
The immediate risk of the operation itself is very low.
-
No organs overlap or are deleted.
-
The ability to easily control the narrowing lumen (this makes it possible to adjust the diameter of the ring to the individual needs of the patient).
-
Complete and easy reversibility of the operation (if necessary or at the request of the patient himself, the bandage can be easily removed, after which the former anatomy of the stomach is immediately restored) .Bandaging can easily be converted into any other bariatric surgery (if for some reason the patient is not satisfied with the results of bandaging or the quality of life with a bandage).
Disadvantages of gastric band surgery compared to other bariatric surgeries
Nutritional discomfort-
The feeling of fullness that should occur when food is held over the bandage is characterized by many patients as a feeling of "getting stuck".
-
inability to fully adapt to the new rules of nutrition after gastric bandaging.
the occurrence of almost daily vomiting in response to a violation of the rules of nutrition during gastric banding.
A large number of different "minor" complications that occur throughout life related to the presence of a foreign body in the body. Such complications include:-
Inversion of the adjustment port.
-
Depressurization of the bandage system.
-
Downward displacement of the bandage.
-
Expansion of the small ventricle above the annulus.
-
Suppuration in the area of the control port or the entire system.
-
Expansion of the esophagus and even the gradual migration of the ring into the lumen of the stomach*.
* The last two complications are a consequence of the "overstretching" of the bandage, i.e. they occur when the adjusting cuff of the ring is tightened too much. According to large statistically reliable studies, it is known that 50% of patients who have a gastric band installed have to undergo repeated corrective operations (restoring the system) or complete removal of the band for various reasons. To be fair, it should be noted that all of these complications are not fatal and can be relatively easily eliminated with repeated surgery.Sleeve gastroplasty
 It is based on the restrictive principle, that is, on the narrowing of the upper gastrointestinal tract to limit food intake.
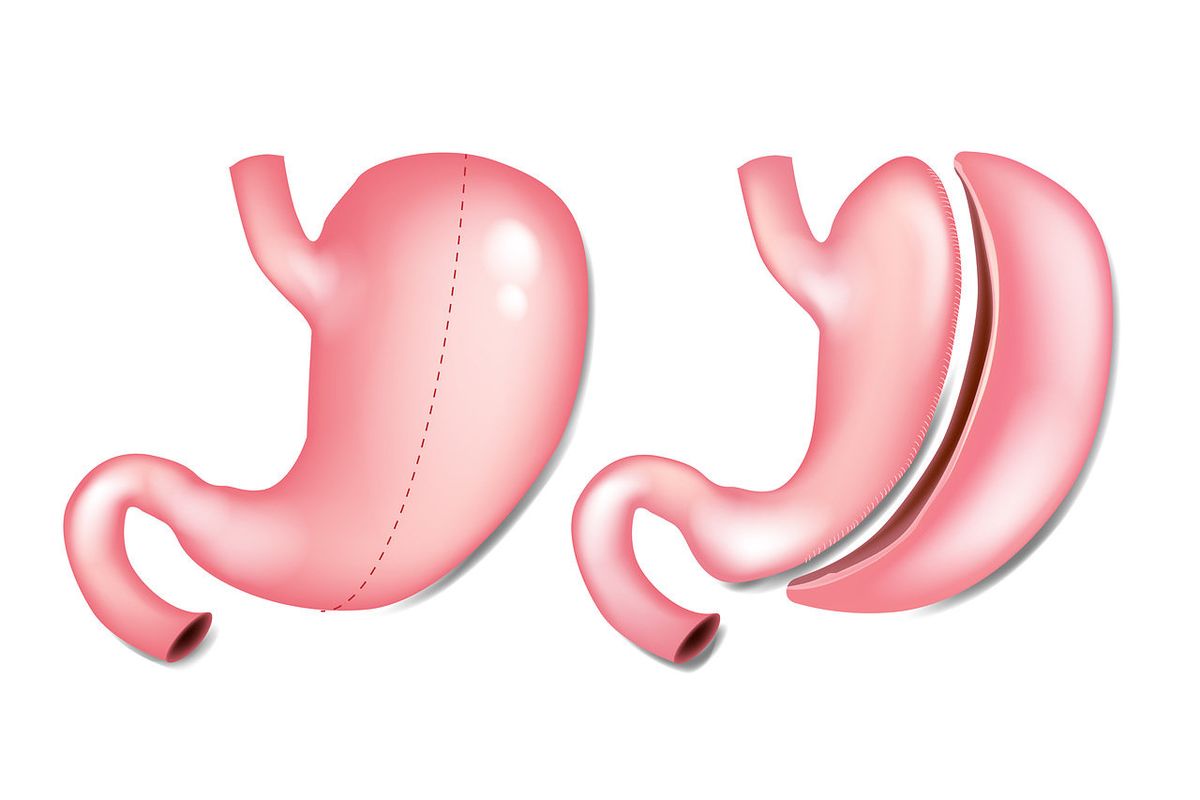
This operation has proven to be an effective method of surgical treatment of overweight, moreover, it has managed to become the world standard, along with gastric banding and gastric bypass surgery.The essence of this intervention is the formation of an extended narrow gastric "sleeve" to obstruct the passage of solid food in the area from the esophagus to the antrum (terminal) part of the stomach.Only a very narrow "sleeve" remains along the small curvature of the stomach, while the bottom and body are completely removed. For crossing and stitching the stomach, as with other bariatric operations, special endosurgical suturing devices and cassettes are used. What is the mechanism of food retention if there is no ring providing a dense local constriction as it progresses? If you remember a little bit of the school physics course, then it's very simple to understand the essence of the phenomenon: the resistance that a liquid experiences passing through a pipeline is directly proportional to the length of the pipeline and inversely proportional to its diameter. Thus, food passing through a long and very narrow "pipeline" overcomes significant resistance and, lingering, causes a persistent feeling of satiety with a very small amount.The history of this operation is interesting. It appeared as the first stage of biliopancreatic bypass surgery in patients with super obesity (180 kg and above). It is known that the risk of prolonged surgery in such patients is very serious, so surgeons tried to break the entire procedure into two short stages.: 1) sleeve resection of the stomach, 2) surgery to move the small intestine, and the second stage was supposed to be performed only a year later, after partial weight loss.Imagine the surprise of the surgeons when it turned out that the effect of the "first stage" was as strong as in such a classic bariatric operation as gastric bypass surgery. The second stage of surgery was not required in these patients, the intestines of the operated patients remained unaffected and the risk of developing a deficiency of protein, calcium, iron, vitamins and other trace elements no longer clouded the immediate life prospects of the patients.
It is based on the restrictive principle, that is, on the narrowing of the upper gastrointestinal tract to limit food intake.
This operation has proven to be an effective method of surgical treatment of overweight, moreover, it has managed to become the world standard, along with gastric banding and gastric bypass surgery.The essence of this intervention is the formation of an extended narrow gastric "sleeve" to obstruct the passage of solid food in the area from the esophagus to the antrum (terminal) part of the stomach.Only a very narrow "sleeve" remains along the small curvature of the stomach, while the bottom and body are completely removed. For crossing and stitching the stomach, as with other bariatric operations, special endosurgical suturing devices and cassettes are used. What is the mechanism of food retention if there is no ring providing a dense local constriction as it progresses? If you remember a little bit of the school physics course, then it's very simple to understand the essence of the phenomenon: the resistance that a liquid experiences passing through a pipeline is directly proportional to the length of the pipeline and inversely proportional to its diameter. Thus, food passing through a long and very narrow "pipeline" overcomes significant resistance and, lingering, causes a persistent feeling of satiety with a very small amount.The history of this operation is interesting. It appeared as the first stage of biliopancreatic bypass surgery in patients with super obesity (180 kg and above). It is known that the risk of prolonged surgery in such patients is very serious, so surgeons tried to break the entire procedure into two short stages.: 1) sleeve resection of the stomach, 2) surgery to move the small intestine, and the second stage was supposed to be performed only a year later, after partial weight loss.Imagine the surprise of the surgeons when it turned out that the effect of the "first stage" was as strong as in such a classic bariatric operation as gastric bypass surgery. The second stage of surgery was not required in these patients, the intestines of the operated patients remained unaffected and the risk of developing a deficiency of protein, calcium, iron, vitamins and other trace elements no longer clouded the immediate life prospects of the patients.The place of sleeve gastroplasty among other modern bariatric operations
Advantages of sleeve gastroplasty:-
The effect of sleeve gastroplasty surgery in terms of weight is approaching gastric bypass surgery.
-
No need for corrective measures in the postoperative period (the operation is similar to gastric bypass surgery – "done and forgotten").
-
Absence of a foreign body in the body.
-
The possibility to "suture" the gastric tube, if necessary, if the effect of the operation is assessed as "insufficient" in the future.
-
The possibility, if necessary, to convert sleeve gastroplasty into gastric or biliopancreatic bypass surgery (for this you just need to supplement the operation with an "intestinal stage").The most "trouble-free" operation in the long term (surgery-related complications are less likely to occur after it).However, the effectiveness of the operation does not yet indicate that it should be performed by everyone, discarding all the long-term experience of bariatric surgery. Like all other operations, this intervention, along with its undeniable advantages, has a number of disadvantages.Disadvantages of sleeve gastroplasty:
-
The only irreversible bariatric surgery.
-
Has a higher initial surgical risk compared to gastric bandaging (the risk is associated with the need to cross and remove part of the stomach). To prevent the development of early complications, the hospital stay of operated patients is 4 days (after gastric bandaging, only 1 day).
-
In the part of the stomach that is being removed, there is a zone of production of the so-called internal factor Castle. It is a protein that binds to vitamin B12 and ensures its absorption into the blood from the gastrointestinal tract. In most cases, the remaining stomach is sufficient to meet the body's needs for this protein, however, the so-called B12 deficiency anemia (i.e., a decrease in blood hemoglobin) may develop. In case of this problem, it is necessary to take vitamin B12.
-
According to the literature, almost 50% of patients who have undergone sleeve gastroplasty develop heartburn.
The results of operations performed before 2010 were the same. This led to a change in the technique of performing the operation. Now we are preserving the natural valve between the esophagus and the stomach, which has led to a reduction in the frequency of this problem by almost 10 times.Thus, currently in our practice, 5% of patients have heartburn. Nevertheless, it is impossible to exclude a situation where constant intake of medications for heartburn is required.
Why the EMС
The first and only clinic in Russia, created in the image of the world's leading clinics


Get help
Specify your contacts and we will contact you to clarify the details.
Doctors

Chzhao Аleksey
Doctor of Medicine, Professor
-
Chzhao Аleksey
Doctor of Medicine, Professor
- One of the world's leading specialists in the field of abdominal and, in particular, hepatopancreatobiliary surgery, the creator of new directions in surgical hepatology and pancreatology
- He contributed to the organization and development of a modern liver transplantation service in Moscow and the Russian Federation
- He founded the transplantation program at the Moscow City Liver Transplantation Center at the N.V. Sklifosovsky Research Institute of Joint Venture
Total experience
44 years
Experience in EMC
since 2022
