

Balloon angioplasty and stenting technique
 The essence of balloon angioplasty is that a specially selected balloon catheter is inserted into the narrowing area. By inflating it under pressure (6-14 atm), it is possible to eliminate the narrowing of the vessel in 96-98% of cases. After that, 80% of patients who follow preventive measures forget about angina pectoris for many years. Then a metal tubular frame – a stent - is implanted in the narrowing area. This procedure is called stenting of the heart vessels.
The essence of balloon angioplasty is that a specially selected balloon catheter is inserted into the narrowing area. By inflating it under pressure (6-14 atm), it is possible to eliminate the narrowing of the vessel in 96-98% of cases. After that, 80% of patients who follow preventive measures forget about angina pectoris for many years. Then a metal tubular frame – a stent - is implanted in the narrowing area. This procedure is called stenting of the heart vessels.
Balloon angioplasty is currently not used in isolation (because stenting is dozens of times more effective) and can be used both before stenting to prepare the lesion for stent implantation, and after it to ensure a tighter fit of the stent to the vessel wall in the case of anatomical features of the artery at the stenting site.
Routine and emergency stenting
Stenting can be "planned" or "emergency".
As the name suggests, "emergency" stenting is performed in critical conditions when it is necessary to eliminate narrowing/occlusion of the coronary artery as soon as possible in order to either protect the heart from a heart attack or limit the area of infarction in case of its development. And the sooner and more fully the blood flow through the arteries of the heart is restored in such a patient, the more chances he has for salvation and an uncomplicated and favorable course of a heart attack.
"Elective" stenting has the advantages of a longer time interval for an adequate assessment of the nature of coronary artery lesions, choosing the most optimal treatment strategy for the patient and carefully preparing him for the stenting procedure, minimizing the risks of intervention.
If the atherosclerotic process is diffuse, multiple in nature, then intravascular methods are powerless or have significantly lower effectiveness. In these cases, patients are recommended to consult a cardiac surgeon to resolve the issue of the possibility of coronary artery bypass surgery (CABG), when the surgeon sews a new vessel to the heart, the so—called shunt, thereby eliminating the nutritional deficiency of the heart muscle.
Indications for angioplasty and stenting
Indications for balloon angioplasty and stenting are the following conditions:
- First-time and progressive angina pectoris with pain in the chest that occurs during physical exertion and passes at rest
- Acute myocardial infarction (AMI) is a sharp pain in the chest that persists after taking nitropreparations
- Early postinfarction angina pectoris or persistent attacks of chest pain after acute myocardial infarction
- Stable angina pectoris, if the patient's quality of life does not suit him (pain that occurs during exercise, preventing the patient from living a full life) Painless myocardial ischemia is a condition when a patient does not feel angina pectoris, but according to cardiological studies, he has signs of significant myocardial ischemia.
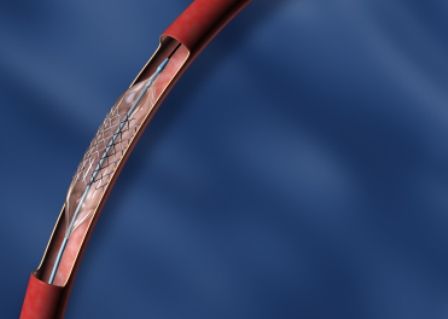
Types of stents
Currently, there are basically two types of stents — with and without a drug coating, the so-called. holometallic stents.
In our clinic, we use the full range of stents available on the market, but we prefer the latest (IV) generation of drug-coated stents, which have proven to be highly effective in terms of safety and long-term results compared to holometallic stents..
There are also biodegradable frameworks, the main feature of which is the ability to completely dissolve after the function has been performed. Unfortunately, at the current stage of development of this technology, many questions remain, and clinical research data do not indicate the unconditional superiority of bio-soluble stents over drug-coated stents. However, there are some clinical situations (a young patient, a small and undeveloped area of arterial lesion, etc.) when this technology can be successfully applied.
Angioplasty and stenting procedure
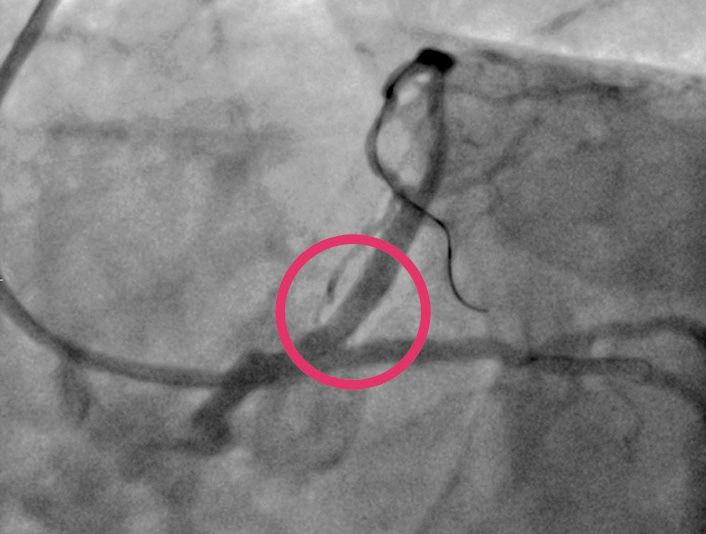
The stenting procedure can be either an independent procedure or a continuation of diagnostic coronary angiography. The decision is made taking into account all the risks, the features of the anatomy of the vascular bed, the complexity of the lesion and the amount of contrast agent used. The choice of a stent is also carried out by analyzing many factors: the type and nature of the vessel lesion, anatomical features, since the tortuosity of the vessel, its diameter and extent of the lesion, the location of large lateral branches in the affected area, previous interventions in the area of interest, etc. Depending on the number of implantable stents and possible anatomical features, the procedure can last from 20-30 minutes to 2-3 hours. Stenting does not require anesthesia, as the procedure itself is safer than general anesthesia. Restoration of blood supply in the coronary artery:

Rehabilitation after angioplasty with stenting
After the intervention, the patient can be transferred to the intensive care unit if the stenting was performed for "emergency" indications or simply to his room with mandatory monitoring of hemodynamic parameters. If the intervention was performed through femoral access, the patient is prescribed strict bed rest. In the case of transradial access, bed rest is limited to 2-4 hours. In our practice, we try to maximize the use of "over-the-arm" access for greater patient comfort. After a "routine" stenting procedure, in the absence of complications and complaints, the patient can be discharged home the next day. No special rehabilitation period is required. The attending cardiologist will provide all the information on the motor and drug regimen for each patient, taking into account his individual characteristics.
Advantages of balloon angioplasty and stenting in EMC
- The hospital of the European Medical Center at 35 Shchepkina St., Moscow, houses a modern X-ray surgical operating room equipped with the innovative ARTIS zee biplane angiographic system (Siemens).
- The Clinic employs highly qualified endovascular surgeons with many years of experience in Russia and abroad and performing interventions of any complexity.
- We use the full range of modern stents of the latest generation.






















