Rectal prolapse
Rectal prolapse is one of the most serious diseases of the rectum, as it results in the exit of all layers of the rectum through the posterior opening.
When the rectum prolapses, compression of the vessels of the submucosal layer is observed, as a result of which the mucous membrane acquires a blue hue and may die (necrotize) as a result of prolonged compression from the walls of the anal canal. After reduction of the intestine, the mucous membrane acquires a normal appearance, as the blood flow is fully restored.
With internal prolapse of the rectum, a solitary ulcer develops, forming on the anterior wall of the rectum due to damage to the wall when the intestine is screwed in. Note that instead of a solitary ulcer, redness (hyperemia) and focal edema may develop on the anterior wall of the rectum.
Causes of rectal prolapse
As a rule, the cause of rectal prolapse is a combination of adverse circumstances, however, in most patients, the leading etiological factor can be identified.
Predisposing causes include constitutional and anatomical features of the body and rectum, a hereditary factor, as well as acquired degenerative changes in the wall of the rectum and in the muscles of the locking apparatus. The immediate causes of rectal prolapse include:
-
severe diarrhea;
-
disorders of emptying of the rectum, accompanied by prolonged straining for emptying;
-
inadequate emptying efforts (central nervous system dysfunction);
-
dramatic weight loss;
-
prolonged heavy physical activity;
-
blunt abdominal injuries (with a sharp increase in intra-abdominal pressure, the rectum turns outward through the anus, like a hernia).
Relatively rare causes are homosexuality, self-mutilation, pelvic organ surgery, etc .
Intestinal dysfunction, neurological changes, that is, senile changes, spinal cord injury, damage to the tail of the spinal cord, and sudden weight loss contribute to the development of the disease.
Symptoms of rectal prolapse
The main symptom of the disease is partial or complete prolapse of the rectum. The second most common symptom observed in 80% of patients is incontinence of intestinal contents due to weakness of the rectal sphincter. 50% of patients have impaired colon function, usually in the form of bowel movement disorders (constipation).
The pain syndrome is not pronounced and is noted only with sudden prolapse of the rectum. It should be noted that half of the patients report pain in the lower abdomen, which increases with defecation, walking and significant physical exertion.
Patients often complain of abnormal discharge from the anus (bloody or in the form of mucus) caused by injury to small vessels of the mucous membrane. Other complaints include false urge to defecate and a feeling of a foreign body in the rectum.
Degrees of rectal prolapse:
Grade I – prolapse occurs only during bowel movements;
Grade II – prolapse occurs during bowel movements and physical exertion;
Grade III – prolapse occurs when walking.
Diagnosis of rectal prolapse
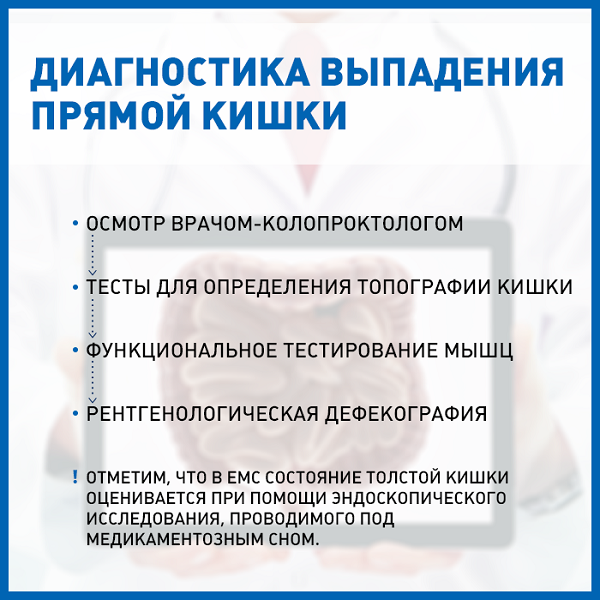
The standard diagnosis for rectal prolapse is an examination by a coloproctologist, who conducts special tests to determine the topography of the protruding object (the shape and size of the protruding part of the rectum, the height from which rectal prolapse begins, the condition of the mucous membrane and dentate line, the presence of a solitary ulcer of the rectum).
Functional testing of the muscles compressing the anus and perineal muscles is also performed to assess their condition. Then an X-ray defecography is performed, which examines the parameters of emptying the rectum, the presence of weak spots in the walls of the pelvic organs, the size of the perineal prolapse, indicating relaxation of the muscular framework and connective tissue structures supporting the rectum and the rest of the pelvic organs. The data obtained in this study makes it possible to clarify the scope of the operation.
Note that the condition of the colon is assessed using an endoscopic examination performed under medication.
Treatment of rectal prolapse
Currently, surgical treatment of rectal prolapse is mainly used in adults. Conservative therapy is possible in children.
The most popular operation is laparoscopic fixation of the prolapsed intestine to the periosteum of the upper third of the sacrum (according to the type of Ripstein's operation). In patients with concomitant fecal incontinence, sphincterolevatoroplasty can be performed simultaneously with presacral rectopexy, however, this operation can often be performed in the second stage after a while in order to evaluate the possibilities of independent recovery of the perineal and anus muscles from specialized gymnastics.
In patients with severe elongation of the sigmoid colon and the presence of constipation against the background of this disease, it is possible to remove excess sigmoid colon with anastomosis (stitching of the ends of the intestine) to prevent postoperative constipation.
Rectal prolapse is very common in women with a herniated rectovaginal septum – rectocele. In elderly patients, operations are possible only from the side of the perineum according to the type of Altmaier or Delorme surgery.
Often, this disease is combined with perineal prolapse and solitary ulcer syndrome of the rectum.In this case, the treatment of rectal prolapse is carried out jointly with specialized specialists, for example, with a gynecologist .
Why the EMC
The first and only clinic in Russia, created in the image of the world's leading clinics


.webp)







.webp)

.webp)
.webp)





.webp)


Make an appointment for a consultation
Specify your contacts and we will contact you to clarify the details

and new products of the EMC