Lung cancer, or bronchogenic carcinoma, is a malignant neoplasm originating from the tissue of the bronchi or pulmonary parenchyma. Lung cancer is one of the most common cancers in men and women worldwide.
Types of lung cancer
-
Small cell lung cancer (SCLC) is diagnosed in 10-15% of patients. It tends to have a more aggressive course, rapid spread, and relapses.
-
Non-small cell lung cancer (NSCLC) includes all other types of lung cancer and is diagnosed in 85-90% of patients. NSCLC has subcategories, the most common of which are adenocarcinoma and squamous cell carcinoma. This type of lung cancer is often an indication for surgical treatment, especially in the early stages of the disease.
Small cell and non-small cell lung cancer suggest different approaches to surgical treatment, radiation and chemotherapy. Until recently, a simple histological separation of NSCLC and MCLC, along with the stage, was adequate for deciding on treatment when lung cancer was diagnosed for the first time. Today, it has already been proven that in order to determine optimal therapy, it is important to distinguish between adenocarcinoma, squamous cell carcinoma and other histological forms of the tumor.
Symptoms of lung cancer
In the early stages of the disease, in which treatment will be most effective, symptoms are insignificant and absent, which underlines the relevance of screening studies in patients with high cancer risk.
The most common clinical manifestations of lung cancer are:
-
Cough occurs in 50-75% of patients
-
Hemoptysis occurs in 25-50% of patients
-
Dyspnea occurs in 25% of patients
-
Chest pain – in 20% of patients
The appearance of symptoms, as a rule, indicates a far-reaching process.
Less often, lung cancer can manifest as abnormalities in laboratory parameters due to metastasis to other organs (most often to the liver, bones, brain) or paraneoplastic syndrome – this is a complex of manifestations not directly related to the tumor, but caused by the effects of cancer cells on the body.
Paraneoplastic syndrome includes:
-
hypercalcemia (increased concentration of calcium in blood plasma),
-
Cushing's syndrome (increased secretion of the hormone cortisol by the adrenal cortex),
-
hypercoagulable disorders (increased blood clotting),
-
various neurological syndromes (coordination disorders, balance problems, difficulty walking, difficulty speaking, swallowing, etc.).
Small cell and non-small cell lung cancer may exhibit the same symptoms. But small cell carcinoma is characterized by:
-
rapid progression of symptoms,
-
paraneoplastic syndrome,
-
volumetric multiple metastases in mediastinal lymph nodes,
-
superior vena cava syndrome,
-
bone metastases and brain metastases.
Whereas Pancost syndrome (weakness and pain in the arm caused by the growth of a tumor of the upper lobe of the lung into the brachial plexus) and hypercalcemia are more often found in patients with non-small cell lung cancer.
Lung cancer diagnosis

A patient with suspected lung cancer is assigned computer topography (CT)thoracic cavity and upper abdominal cavity (usually with contrast) to assess the extent of the primary tumor and possible spread to the mediastinum, liver and adrenal glands.
The final diagnosis of cancer is established only on the basis of cytological examination (for example, pleural fluid) or histological examination (tissue biopsy).
A biopsy can be performed using one of the following methods:
-
Bronchoscopy
-
Endobronchial ultrasound bronchoscopy, or EBUS, is a technique that combines the use of a flexible bronchoscope with ultrasound
-
Fine needle biopsy under CT control
-
Needle aspiration
-
Thoracocentesis
- In the event that other biopsy procedures have failed to determine the diagnosis, surgery may be required. The most common surgical procedures are mediastinoscopy, which is used to biopsy the lymph nodes in the central part of the chest cavity; video-assisted thoracoscopic surgery (VATS), a less invasive method for lung tissue biopsy; and thoracotomy, which is a cavity surgery to remove large parts of lung tissue or tumors.
Radiologist, specialist in cancer diagnostics at the EMC Institute of Oncology Professor Evgeny Libson (Israel) has many years of experience in performing fine-needle CT-controlled biopsies, which allows many patients to avoid open surgery performed for diagnostic purposes.
After the biopsy, the material is sent to the EMC Histological Laboratory to establish an accurate diagnosis and obtain important tumor characteristics that help in further treatment selection.
If necessary or at the request of the patient, the diagnosis is verified in leading clinics in the USA, Great Britain, Israel, Germany, France, Switzerland (using telepathology). Getting a "second opinion" from a foreign specialist is included in the standard cost of the study.
Molecular analysis of the tumor
The EMC Institute of Oncology also performs molecular analysis of the tumor to identify specific tumor biomarkers or gene mutations. This allows you to create a so-called "molecular portrait" of the tumor and perform targeted drug therapy, which has a better effect than standard chemotherapy. The most common biomarkers of lung cancer are EGFR mutations, ALK translocations, and c-ROS oncogene 1 (ROS1 oncogene) translocations.
Staging
 After the diagnosis is established, it is necessary to conduct a follow-up examination for the correct staging of the disease. For this purpose, the following may be assigned:
After the diagnosis is established, it is necessary to conduct a follow-up examination for the correct staging of the disease. For this purpose, the following may be assigned:
-
Ultrasound examinations of the pleural and abdominal cavities, blood vessels, and lymph nodes (to diagnose the spread and complications caused by the tumor)
-
MRI of the brain (in the presence of neurological symptoms)
-
X-ray of the pelvic region (for pelvic pain)
-
Echocardiography to assess malignant pleural effusion (in the presence of hypotension with sinus tachycardia).
Laboratory tests
If lung cancer is suspected, the following CT scans are performed:
-
General blood test
-
Electrolytes
-
Calcium
-
Alkaline phosphatase
-
ALT, AST, total bilirubin
-
Creatinine
-
Total protein, albumin and lactate dehydrogenase (optional)
-
Coagulogram
Clinical examination and laboratory tests are performed to identify possible metastases. Deviations of laboratory parameters from the norm are the basis for the appointment of additional instrumental studies.
EMC uses a modern high—precision method for staging lung cancer - PET/CT scan of the whole body. PET / CT is performed in patients with stage I, II and III of the disease, it is mandatory to conduct a study before surgery. PET/CT can detect tumor foci in the lymph nodes that are not detectable by CT, as well as distant metastases in other organs. The initial stage and treatment tactics are often reviewed based on PET/CT results.
The stages of non-small cell lung cancer are determined based on the following factors:
-
the size and location of the tumor
-
the spread of the tumor to the lymph nodes and tissues inside the chest cavity
-
the spread of the tumor beyond the chest cavity (for example, lung cancer can metastasize to bones, liver, adrenal glands or other organs).
The stages of non-small cell lung cancer range from I to IV:
-
Stage I – the diameter of the tumor is less than or equal to 3 cm, the tumor has not spread to any other tissues or lymph nodes.
-
Stage II – Stage II means that the tumor has a size from 3 to 7 cm or has spread to the lymph nodes, or has penetrated into the tissues surrounding the lung, or has begun to grow into the bronchial lumen.
-
Stage IIIA – Stage IIIA of the disease means that the tumor can be larger than 7 cm or spread to the lymph nodes in the center of the chest cavity (mediastinum), or has grown into the ribs, heart, esophagus or trachea.
-
Stage IIIB – Stage IIIB of the disease means that the tumor has spread to lymph nodes outside the mediastinum or to lymph nodes above or below the collarbone. Stage IIIB also includes tumors that have spread to the ribs, heart, esophagus or trachea without involving the lymph nodes of the mediastinum.
-
Stage IV – Stage IV means that the cancer has spread beyond the chest cavity or to the opposite side of the mediastinum. In stage IV, cancer can lead to an accumulation of fluid around the lung or heart (malignant effusion).
Stages of small cell lung cancer . The technical separation of small cell carcinoma at the stage is exactly the same as for non-small cell carcinoma. However, treatment options are usually determined by a simpler scheme. Small cell lung cancer is usually characterized as a "limited" or "widespread" process.
-
a limited process is small cell lung cancer, which is limited to one side of the chest cavity and the lesion of regional lymph nodes.
-
a common process is small cell lung cancer that has spread to the opposite side of the chest and other organs outside the chest.
Lung cancer treatment
 The EMC Institute of Oncology has all the capabilities to provide care to patients with lung cancer according to international standards.
The EMC Institute of Oncology has all the capabilities to provide care to patients with lung cancer according to international standards.
Lung cancer treatment in EMC:
-
An international team of doctors: specialists with experience in the USA, Israel, and Western Europe.
-
Each clinical case is discussed in a multidisciplinary consultation. A team of specialists, including oncologists, surgeons, radiologists, morphologists, and radiation therapists, determines treatment tactics individually for each patient.
-
Comprehensive diagnostics (CT, MRI, PET/CT)
-
Chemotherapy according to modern European and American protocols, the latest generation of drugs from the world's leading manufacturers.
-
Targeted therapy based on molecular tumor analysis
-
Immunotherapy
-
The latest systems for radiation therapy and stereotactic radiation therapy Varian EDGE, Truebeam, USA.
-
Psychotherapeutic support for the patient and his family.
Early stages of lung cancer are usually amenable to surgical treatment by removing the tumor and surrounding lung tissue. Stage III lung cancer is often treated with a combination of chemoradiotherapy and surgery at various stages of therapy. If the cancer has spread beyond the chest cavity (stage IV), chemotherapy and radiation therapy are used to control the disease and its symptoms.
Systemic chemotherapy is one of the most important components of treatment for patients with MCRL, as almost all patients already have advanced MCRL at the time of treatment. For patients with a limited stage, radiation therapy of the thoracic cavity is used in combination with chemotherapy. Preventive radiation therapy is often performed on the brain to reduce the incidence of brain metastases and increase survival. Preventive radiation therapy in the head and chest area may also have a positive effect in patients with a complete or partial response to primary systemic chemotherapy.
Surgical treatment of lung cancer

Surgical resection provides the best long-term survival and often complete cure in patients with non-small cell lung cancer. However, even if there is a tumor that can be removed, the patient may be "inoperable" due to insufficient lung function or due to concomitant diseases, therefore, a comprehensive examination is of great importance in preparing for surgery.
Surgical interventions in patients with suspected or diagnosed lung cancer may vary in scope and goals that need to be achieved as a result of surgery. The prediction of the surgery volume is based on the results of the examination and the joint decision of the interdisciplinary EMC council.
If lung cancer is suspected and it is not possible to take material for histological examination, diagnostic surgery may be necessary:
- Biopsy of mediastinal lymph nodes.
It is performed using modern minimally invasive technologies – videomediastinoscopy or videothoracoscopy with small surgical incisions (1-2 cm) and minimal injury to muscles and other tissues. The operation is usually well tolerated, the duration of hospitalization rarely exceeds 2-3 days.
It can also be performed by video thoracoscopic access.
There are surgical interventions aimed at removing the pleura or inducing pleurodesis (an adhesive process in the pleural cavity). Performing such operations helps to stop complications associated with pleural metastasis and the development of recurrent pleurisy. Such complications can not only interfere with chemotherapy, but also be life-threatening.
The choice of the method of radical surgical treatment of lung cancer depends on the location of the tumor, its size, signs of germination of neighboring structures and damage to the lymph nodes. The following can be distinguished by volume operations:
If lung cancer is detected at an early stage, when there is no germination of neighboring organs and the tumor size is less than 5-6 cm, it is possible to perform surgery with minimally invasive access using video thoracoscopy and small incisions.
Radiation therapy of lung cancer in EMC
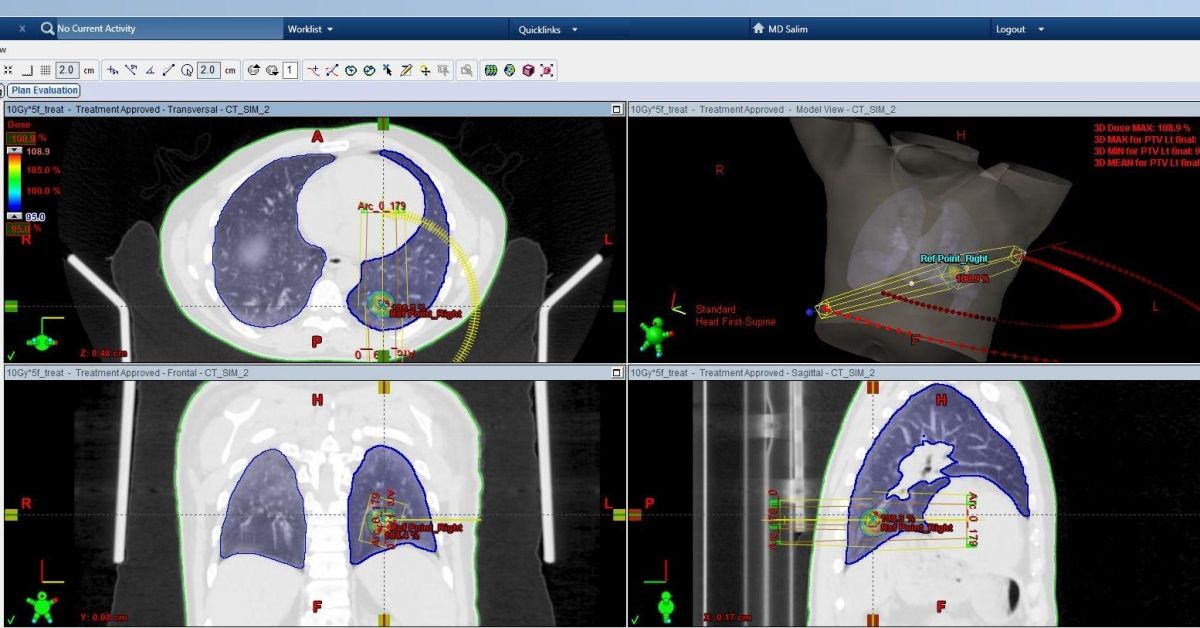
Stereotactic radiosurgery SBRT (Stereotactic Body Radiation Therapy), also known as SABR (Stereotactic Ablative Body Radiotherapy) is an effective and safe non-invasive method for the treatment of stage 1 non-small cell lung cancer, that is, tumors up to 5 cm in size and with intact lymph nodes). Studies have shown equivalent overall survival and local tumor control when comparing surgery (lobectomy, the current standard of treatment) and SBRT in elderly or inoperable patients with concomitant pathology.
3 to 5 sessions (fractions) of SBRT are used.
The EMC Radiation Therapy Center, led by the chief radiotherapist of Moscow, Dr. Nidal Salim, is one of the few radiotherapy departments in the world where stereotactic radiosurgery is used in the treatment of primary and metastatic tumors of the lung, liver, prostate and pancreas, brain and spinal cord and bones. The Center has the latest EDGE and Truebeam radiation therapy systems from the USA, which allow the use of the most modern methods of radiation treatment.
Modern technologies in radiation therapy, such as IMRT, VMAT/RapidArc, and IGRT, make it possible to increase the accuracy of radiation and preserve healthy tissues surrounding the tumor.
When lung tumors are irradiated, especially those localized in the lower lobes, there is a high mobility of the focus at different phases of respiration. The use of Gated RapidArc technology makes it possible to irradiate a tumor, taking into account its actual deviation at all phases of respiration, or temporarily stop irradiation when inhaling/exhaling beyond a set interval.
Pancost tumor treatment
Pancost tumor (tumor of the upper sulcus of the lung) refers to non-small cell lung cancer, which is located in the upper part of the lung. The tumor affects the nerves, causing characteristic symptoms such as:
As the tumor progresses, the eyelid droops (ptosis), and sweating on the affected side stops completely. In the absence of separated metastases, Pancost tumor treatment consists of chemoradiotherapy and subsequent surgery.
Treatment of stage IV lung cancer
Patients with stage IV of the disease usually receive treatment with systemic agents or symptomatic palliative therapy. In properly selected patients, chemotherapy, molecular targeted therapy, and/or immunotherapy can increase survival without compromising quality of life. For some patients, it is advisable to undergo radiation therapy and surgery as a symptomatic palliative treatment.
In patients with stage IV disease with distant metastases (for example, in the brain, adrenal glands), resection of metastases, as well as aggressive treatment of the primary tumor, may have a beneficial effect.
The EMC Institute of Oncology has created all the possibilities for providing care to patients with metastatic lung cancer, including the use of the latest immunotherapy drugs (Nivolumab, Pembrozilumab), which have demonstrated effectiveness in increasing survival in patients with stage IV of the disease.
Palliative therapy is used to improve the quality of life of patients with stage IV of the disease. We provide all necessary assistance to seriously ill patients, including adequate anesthesia, palliative surgery and radiation therapy, including in an emergency mode. Dyspnea resulting from full involvement of the central respiratory tract may be amenable to palliative treatment by removing the tumor using a rigid or flexible bronchoscope and laser coagulation or cryotherapy. Stenting may be required to maintain airway patency and to create conditions for external radiotherapy.
Prognosis for lung cancer
For patients with non-small cell lung cancer, the factor that has the greatest impact on prognosis is the TNM stage at the time of treatment. Survival progressively decreases with a higher degree of the disease, averaging from 59 months for patients with stage IA of the disease to four months for patients with stage IV.
Clinical signs at the time of diagnosis also make it possible to predict survival, regardless of the stage of the disease. Most of these factors were identified in studies that predominantly included patients with progressive or inoperable forms of NSCLC. It has been found that low performance and weight loss are associated with reduced survival. Decreased appetite, a factor preceding weight loss, also has a negative prognostic value.
The most important prognostic factor in patients with MCRL is the prevalence of the disease at the time of treatment. For patients with limited stages of the disease, the average life expectancy ranges from 15 to 20 months, with a five-year survival rate of 10-13%. For patients with advanced stages of the disease, the average life expectancy is 8-13 months, and the five—year survival rate is 1-2%. It should be borne in mind that these are average statistical indicators, the forecast is different in each individual case.
Risk factors
Among all the risk factors for lung cancer, smoking plays a leading role, which is "responsible" for 90% of lung cancer cases. A person who smokes a pack of cigarettes a day for 40 years has a 20-fold higher risk of developing lung cancer than a non-smoker. The presence of other carcinogenic factors, such as exposure to asbestos, further increases the risk of disease.
Quitting smoking reduces the likelihood of developing the disease, especially for those who quit smoking before the age of 30. But former smokers have a higher risk of developing lung cancer with age than those who have never smoked.
Among other proven risk factors:
-
Radiation therapy for the lung area. The risk of developing lung cancer is higher in patients who previously underwent radiation therapy for another cancer (in particular, in patients who underwent radiation therapy for breast cancer and Hodgkin's lymphoma)
-
Exogenous toxins (asbestos, radon, arsenic, chromium, nickel, ionizing radiation, polycyclic aromatic hydrocarbons, and secondhand smoke).
-
Pneumosclerosis (pulmonary fibrosis) – according to the results of several studies, the risk of developing lung cancer is about seven times higher in patients with pulmonary fibrosis.
-
HIV infection
-
Genetic predisposition
The role of alcohol in the development of lung cancer requires further study. Attempts to reduce morbidity in high-risk groups with the help of a diet (antioxidants, phytoestrogens) have not yet been successful. On the contrary, one study proved that the intake of beta-carotene in vitamin preparations by smokers led to an increase in morbidity.
Lung cancer screening
Screening is a study that allows you to identify diseases before symptoms appear. Until recently, lung cancer screening was not widespread, as several studies have shown that chest X-rays and sputum cytology did not lead to a reduction in lung cancer mortality.
Over the past few years, more accurate research methods have emerged, such as low-dose computed tomography of the lungs. The radiation load during this study is 5-10 times less than that of a standard CT scan, which allows the method to be used as screening.
As a result of a major study conducted by the US National Cancer Institute, it was found that low-dose CT scans performed on experienced smokers reduced lung cancer mortality by 20% compared with smokers who underwent chest X-rays in a similar mode.
To date, this method has been recommended by the United States Preventive Service Task Force (USPSTF) for lung cancer screening for people aged 55 to 80 years who have a 30—year history of smoking or quit smoking no more than 15 years ago.
EMC was one of the first centers in Russia to introduce low-dose CT of the lungs for early diagnosis of lung cancer.



.webp)